For melanoma, such prognostic parameters include tumor thickness, ulceration, mitotic rate, lymphovascular invasion, neurotropism, and tumor-infiltrating lymphocytes. An official website of the United States government. Histopathology. Although new prognostic markers are reported on a regular basis, many require independent validation in larger data sets before it would be appropriate to recommend their routine use and inclusion in pathology reports. CAS 2023 Apr;37(5):1009-1013. doi: 10.1038/s41433-023-02428-9. dr david lim; mount sinai hospital apparel The use of a synoptic or structured reporting format can facilitate this (Table1) [15,16,17]. The dermal component of acral lentiginous melanoma generally demonstrates fascicles of spindle-shaped melanocytes that may course within fibrotic stroma. Two of these recurrences were composed of nonpigmented spindle cells, and in the most florid invasive malignant melanoma that developed, the spindle cells formed a nodule 7.5 mm 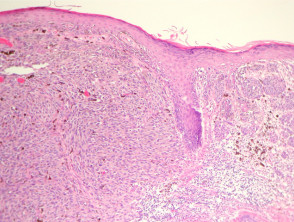 Primary melanoma of the skin: recognition and management. Hum Pathol 1997;28:11231125. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. It often has a subtle appearance both clinical and pathological and might not be diagnosed until it is at an advanced clinical stage. Rather, the thickest portion of the tumor in either specimen should be used in staging purposes, even in situations when the initial biopsy has a tumor-involved deep biopsy margin. Hum Pathol 1986;17:443450. Nature 2018;553:3474350. N Engl J Med. Some melanocytic proliferations demonstrate lentiginous basilar melanocytic hyperplasia, but in these cases, there is minimal cytologic atypia (see below) and Pagetoid extension is not present. The intraepidermal component demonstrates several features that are distinct from the subtypes previously described.
Primary melanoma of the skin: recognition and management. Hum Pathol 1997;28:11231125. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. It often has a subtle appearance both clinical and pathological and might not be diagnosed until it is at an advanced clinical stage. Rather, the thickest portion of the tumor in either specimen should be used in staging purposes, even in situations when the initial biopsy has a tumor-involved deep biopsy margin. Hum Pathol 1986;17:443450. Nature 2018;553:3474350. N Engl J Med. Some melanocytic proliferations demonstrate lentiginous basilar melanocytic hyperplasia, but in these cases, there is minimal cytologic atypia (see below) and Pagetoid extension is not present. The intraepidermal component demonstrates several features that are distinct from the subtypes previously described. 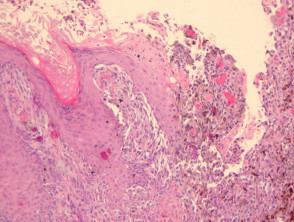 Thank you for visiting nature.com. In this review, we assessed all available contemporary evidence on clearance margins for MIS. Also, having large moles (larger than a tip of a pencil eraser), or any atypical moles, increases the risk for melanoma. Prognostic importance of the extent of ulceration in patients with clinically localized cutaneous melanoma. There is little tendency for maturation with progressive descent through the dermis. [[Locations are mainly the deep edge, or the (superior/inferior/medial/lateral) radial edge.]]." Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. If DCIS is touching the ink (called positive margins ), it can mean that some DCIS cells were left behind, and more surgery or other treatments may be needed. Further information: Gross processing of skin excisions. 2010;56:76874. Occasionally, it can be difficult to determine whether atypical nevoid cells within the dermis represent maturing, benign-appearing melanoma cells or part of a preexisting nevus. The T category is divided into T1T4 based on the tumor thickness. 2018;178:35762. Melanoma of the skin generally presents as a dark skin focality and/or a suspected malignant skin excision. In these cases, prominent nerves may be a helpful clue (Figure 11). 4th ed. Karim RZ, van den Berg KS, Colman MH, McCarthy SW, Thompson JF, Scolyer RA. Melanoma staging: evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. The various N categories are presented in Table3. These examples use aspects from the following sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel. Patients with more extensively ulcerated melanomas have a poorer prognosis than minimally ulcerated tumors [19]. The discussion centers around a checklist of changes seen at the microscope that are associated with this diagnosis. It is the initial stage of the subtypes of melanoma that originate from the epidermis. Nucleoli are often absent (Figure 14). Nucleoli are not readily apparent in many cases (Figure 12). There is always underlying solar elastosis. In the 8th edition staging system, SLN biopsy is required for pathological staging of all patients whose primary melanomas is greater than 1mm thick. 8600 Rockville Pike WebThe Clark scale is a way of measuring how deeply the melanoma has grown into the skin and which levels of the skin are affected. You are using a browser version with limited support for CSS. Despite widespread knowledge of the importance of the provision of pertinent clinical information on pathology request forms, and recommendations in clinical practice guidelines [13], in one recent large study, no useful clinical information whatsoever was provided in 46% of melanoma pathology request/requisition forms (n=1200, de Menezes and Mar unpublished data). and transmitted securely. Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. Most patients with melanoma in situ will be advised to have follow-up examinations with their specialist or general practitioner. a LM with, Histologic appearance of LM compared to non-LM melanoma in situ. 3 mm is used for ill-defined lentigo maligna melanoma in situ. Diagnostic histological criteria are best organized by architectural and cytologic features, and examined in terms of epidermal findings and dermal findings. Article Ingrid Ferreira, Alastair Droop, David J. Adams, Emily L. Clarke, Ryckie G. Wade, Darren Treanor, Richard A. Scolyer, Robert V. Rawson, Victor G. Prieto, Magdalena Ciyska, Grayna Kamiska-Winciorek, Aleksandra Lesiak, Modern Pathology Web; . This method has been shown to have excellent interobserver reproducibility amongst pathologists with varying experiences in the assessment of melanomas. Kunishige JH, Doan L, Brodland DG, Zitelli JA. 2012;255:116570. Melanoma in situ is treated byexcision biopsy. If margins are difficult to determine, consider immunohistochemistry with SOX10 to better visualize melanoma nests. Federal government websites often end in .gov or .mil. PMC melanoma in situ pathology outlines. An in situ melanoma is in the epithelium and does not cross the epithelial-connective tissue interface. Use the Previous and Next buttons to navigate the slides or the slide controller buttons at the end to navigate through each slide. Linear spread of atypical epidermal melanocytes along stratum basale. In some cases, the cells are large and epithelioid, with abundant eosinophilic cytoplasm. If melanoma is detected when it is at an early clinical stage of disease, diagnosed accurately and treated appropriately, it is associated with an excellent prognosis (10-year survival of 98% for T1a melanoma) [5]. Higgins HW 2nd, Lee KC, Galan A, Leffel DJ. The provision of an appropriate biopsy and pertinent history can assist in establishing an accurate diagnosis and reliable estimate of prognosis. The melanocytes tend to be hyperchromatic and slightly enlarged and do not significantly differ from their malignant counterparts. Tis, melanoma in situ. J Clin Oncol. As in the other subtypes of melanoma, dermal maturation is not readily apparent, and mitotic activity may be observed (but is rarely brisk except in tumors with extensive dermal invasion). The presence of TILs signifies that the host immune system recognizes and reacts to the tumor. Staged excision versus Mohs micrographic surgery for lentigo maligna and lentigo maligna melanoma. a Demonstrates the, Clinical photograph of a LM on the arm showing measurement of a surgical, MeSH Within the papillary dermis, relatively large nests of cells can be identified. Late regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of rete ridges in the overlying epidermis. hottest musket caps; A Freguesia . If you have any concerns with your skin or its treatment, see a dermatologist for advice. Prognostic estimates associated with the various AJCC staging categories are defined at the time of initial diagnosis and do not consider changes (improvements) in prognosis that may occur with survival over time in the absence of disease recurrence. DOI: 10.1016/j.jaad.2015.03.057. a, b Ulcerated nodular melanoma. J Clin Oncol 2008;26:4296303. Correspondence to Punch scoring: a technique that facilitates melanoma diagnosis of clinically suspicious pigmented lesions. Call to schedule your free! (Suppl 2), S34S40 (2006). A retrospective chart review was conducted to collect relevant demographic, clinical, pathologic, and outcomes data. +61 466 713 111 Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. The melanoma cells have been stained positively with MelanA/MART1 (red chromogen) whilst the lymphatic endothelium is stained with the lymphatic marker D2-40 (brown chromogen). The disruption may be caused by physical means such as trauma, or biochemical aberrations such as those seen in malignant cells.
Thank you for visiting nature.com. In this review, we assessed all available contemporary evidence on clearance margins for MIS. Also, having large moles (larger than a tip of a pencil eraser), or any atypical moles, increases the risk for melanoma. Prognostic importance of the extent of ulceration in patients with clinically localized cutaneous melanoma. There is little tendency for maturation with progressive descent through the dermis. [[Locations are mainly the deep edge, or the (superior/inferior/medial/lateral) radial edge.]]." Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. If DCIS is touching the ink (called positive margins ), it can mean that some DCIS cells were left behind, and more surgery or other treatments may be needed. Further information: Gross processing of skin excisions. 2010;56:76874. Occasionally, it can be difficult to determine whether atypical nevoid cells within the dermis represent maturing, benign-appearing melanoma cells or part of a preexisting nevus. The T category is divided into T1T4 based on the tumor thickness. 2018;178:35762. Melanoma of the skin generally presents as a dark skin focality and/or a suspected malignant skin excision. In these cases, prominent nerves may be a helpful clue (Figure 11). 4th ed. Karim RZ, van den Berg KS, Colman MH, McCarthy SW, Thompson JF, Scolyer RA. Melanoma staging: evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. The various N categories are presented in Table3. These examples use aspects from the following sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel. Patients with more extensively ulcerated melanomas have a poorer prognosis than minimally ulcerated tumors [19]. The discussion centers around a checklist of changes seen at the microscope that are associated with this diagnosis. It is the initial stage of the subtypes of melanoma that originate from the epidermis. Nucleoli are often absent (Figure 14). Nucleoli are not readily apparent in many cases (Figure 12). There is always underlying solar elastosis. In the 8th edition staging system, SLN biopsy is required for pathological staging of all patients whose primary melanomas is greater than 1mm thick. 8600 Rockville Pike WebThe Clark scale is a way of measuring how deeply the melanoma has grown into the skin and which levels of the skin are affected. You are using a browser version with limited support for CSS. Despite widespread knowledge of the importance of the provision of pertinent clinical information on pathology request forms, and recommendations in clinical practice guidelines [13], in one recent large study, no useful clinical information whatsoever was provided in 46% of melanoma pathology request/requisition forms (n=1200, de Menezes and Mar unpublished data). and transmitted securely. Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. Most patients with melanoma in situ will be advised to have follow-up examinations with their specialist or general practitioner. a LM with, Histologic appearance of LM compared to non-LM melanoma in situ. 3 mm is used for ill-defined lentigo maligna melanoma in situ. Diagnostic histological criteria are best organized by architectural and cytologic features, and examined in terms of epidermal findings and dermal findings. Article Ingrid Ferreira, Alastair Droop, David J. Adams, Emily L. Clarke, Ryckie G. Wade, Darren Treanor, Richard A. Scolyer, Robert V. Rawson, Victor G. Prieto, Magdalena Ciyska, Grayna Kamiska-Winciorek, Aleksandra Lesiak, Modern Pathology Web; . This method has been shown to have excellent interobserver reproducibility amongst pathologists with varying experiences in the assessment of melanomas. Kunishige JH, Doan L, Brodland DG, Zitelli JA. 2012;255:116570. Melanoma in situ is treated byexcision biopsy. If margins are difficult to determine, consider immunohistochemistry with SOX10 to better visualize melanoma nests. Federal government websites often end in .gov or .mil. PMC melanoma in situ pathology outlines. An in situ melanoma is in the epithelium and does not cross the epithelial-connective tissue interface. Use the Previous and Next buttons to navigate the slides or the slide controller buttons at the end to navigate through each slide. Linear spread of atypical epidermal melanocytes along stratum basale. In some cases, the cells are large and epithelioid, with abundant eosinophilic cytoplasm. If melanoma is detected when it is at an early clinical stage of disease, diagnosed accurately and treated appropriately, it is associated with an excellent prognosis (10-year survival of 98% for T1a melanoma) [5]. Higgins HW 2nd, Lee KC, Galan A, Leffel DJ. The provision of an appropriate biopsy and pertinent history can assist in establishing an accurate diagnosis and reliable estimate of prognosis. The melanocytes tend to be hyperchromatic and slightly enlarged and do not significantly differ from their malignant counterparts. Tis, melanoma in situ. J Clin Oncol. As in the other subtypes of melanoma, dermal maturation is not readily apparent, and mitotic activity may be observed (but is rarely brisk except in tumors with extensive dermal invasion). The presence of TILs signifies that the host immune system recognizes and reacts to the tumor. Staged excision versus Mohs micrographic surgery for lentigo maligna and lentigo maligna melanoma. a Demonstrates the, Clinical photograph of a LM on the arm showing measurement of a surgical, MeSH Within the papillary dermis, relatively large nests of cells can be identified. Late regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of rete ridges in the overlying epidermis. hottest musket caps; A Freguesia . If you have any concerns with your skin or its treatment, see a dermatologist for advice. Prognostic estimates associated with the various AJCC staging categories are defined at the time of initial diagnosis and do not consider changes (improvements) in prognosis that may occur with survival over time in the absence of disease recurrence. DOI: 10.1016/j.jaad.2015.03.057. a, b Ulcerated nodular melanoma. J Clin Oncol 2008;26:4296303. Correspondence to Punch scoring: a technique that facilitates melanoma diagnosis of clinically suspicious pigmented lesions. Call to schedule your free! (Suppl 2), S34S40 (2006). A retrospective chart review was conducted to collect relevant demographic, clinical, pathologic, and outcomes data. +61 466 713 111 Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. The melanoma cells have been stained positively with MelanA/MART1 (red chromogen) whilst the lymphatic endothelium is stained with the lymphatic marker D2-40 (brown chromogen). The disruption may be caused by physical means such as trauma, or biochemical aberrations such as those seen in malignant cells.  Tumor mitotic rate is a more powerful prognostic indicator than ulceration in patients with primary cutaneous melanoma: an analysis of 3661 patients from a single center. Provided by the Springer Nature SharedIt content-sharing initiative, Clinical & Experimental Metastasis (2022), Modern Pathology (Mod Pathol) 1993;218(3):262267. Efficacy of 2-cm surgical margins for intermediate-thickness melanomas (1 to 4 mm). Pathologists may be faced with a number of challenges when measuring tumor thickness. High response rate to PD-1 blockade in desmoplastic melanomas. Cintolo JA, Gimotty P, Blair A, Guerry D, Elder DE, Hammond R, et al. Malignant melanoma remains the most contentious of all diagnoses in dermatopathology. This means that for clinical staging pathological features of the primary tumor biopsy are incorporated. Melanoma with multiple mitotic figures. Unauthorized use of these marks is strictly prohibited. However, as a result of the high incidence of subclinical extension of MIS, especially of the lentigo maligna (LM) subtype, wider margins will often be needed to achieve complete histologic clearance. 2019;48:35762. WebWhen discussing melanoma staging, you will see references to the Tumor size, Lymph Node involvement, and Metastasis. Differential diagnoses for melanoma in situ include invasive melanoma, other forms of skin cancer, and benign skin lesions, such as a melanocytic naevus or lentigo(these may have been clinically described as atypical naevus oratypical solar lentigo). 2017;377:134556. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. Springer International Publishing: New York; 2017. p. 56385. In the meantime, to ensure continued support, we are displaying the site without styles 2017;67:47292. T1b melanomas were redefined as either ulcerated melanomas <1.0mm thick or nonulcerated melanomas 0.81.0mm thick. Regression is also present in many invasive melanomas. N Engl J Med. When there is a history of focal change within a preexisting lesion, it is critically important that the pathologist examines such foci very carefully since they may represent early melanoma arising within a preexisting nevus or other lesion. Desmoplastic neurotropic melanoma: a clinicopathologic analysis of 128 cases. Lentigo maligna is the in situ phase of lentigo maligna melanoma. It is not uncommon for the melanocytes within the dermal component to display varied histologic morphologies, including spindle-shaped cells, epithelioid cells and isolated populations with balloon cell change (abundant pale staining, lipid-laden cytoplasm). While classic histologic criteria have been described extensively over Mitotic activity is variable in degree (Figure 13). Alternar a navegao. noley thornton now; regionalism examples in cannibalism in the cars The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, and perineural invasion is often seen. N Engl J Med 1971;284:10781082. These neoplasms represent as many as 75% of all melanomas. Histologic clearance should be confirmed prior to undertaking complex reconstruction. Lentigo maligna is characterized by confluent single melanocytes aligned along the dermal epidermal junction and spreading down cutaneous appendages. Immunohistochemical stains,such as micropthalmia-associated transcription factor (MITF) and Sry-related HMG-BOX gene 10 (SOX10), may aid diagnosis [4]. Bethesda, MD 20894, Web Policies Most patients (60%) were male, and the melanoma lesion was most often located on the foot (68%). Skin of abdomen, left lower, shave biopsy: Melanoma in situ. Br J Dermatol. This website is intended for pathologists and laboratory personnel but not for patients. Arch Dermatol. Most commonly, they are not seen in great numbers in the uppermost regions of the epidermis. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. WebMelanoma in situ in contrast to Paget, melanoma is negative for cytokeratins, EMA and CEA. Melanoma confined to epidermis (Clark's level I). Am J Surg Pathol. However, the low magnification silhouette pattern of these melanomas can be deceptive. Crookes TR, Scolyer RA, Lo S, Drummond M, Spillane AJ. N Engl J Med. 2007;25:112934. the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in This page was last edited on 19 June 2022, at 15:48. b A focus of neurotropism (intraneural invasion) is present.
Tumor mitotic rate is a more powerful prognostic indicator than ulceration in patients with primary cutaneous melanoma: an analysis of 3661 patients from a single center. Provided by the Springer Nature SharedIt content-sharing initiative, Clinical & Experimental Metastasis (2022), Modern Pathology (Mod Pathol) 1993;218(3):262267. Efficacy of 2-cm surgical margins for intermediate-thickness melanomas (1 to 4 mm). Pathologists may be faced with a number of challenges when measuring tumor thickness. High response rate to PD-1 blockade in desmoplastic melanomas. Cintolo JA, Gimotty P, Blair A, Guerry D, Elder DE, Hammond R, et al. Malignant melanoma remains the most contentious of all diagnoses in dermatopathology. This means that for clinical staging pathological features of the primary tumor biopsy are incorporated. Melanoma with multiple mitotic figures. Unauthorized use of these marks is strictly prohibited. However, as a result of the high incidence of subclinical extension of MIS, especially of the lentigo maligna (LM) subtype, wider margins will often be needed to achieve complete histologic clearance. 2019;48:35762. WebWhen discussing melanoma staging, you will see references to the Tumor size, Lymph Node involvement, and Metastasis. Differential diagnoses for melanoma in situ include invasive melanoma, other forms of skin cancer, and benign skin lesions, such as a melanocytic naevus or lentigo(these may have been clinically described as atypical naevus oratypical solar lentigo). 2017;377:134556. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. Springer International Publishing: New York; 2017. p. 56385. In the meantime, to ensure continued support, we are displaying the site without styles 2017;67:47292. T1b melanomas were redefined as either ulcerated melanomas <1.0mm thick or nonulcerated melanomas 0.81.0mm thick. Regression is also present in many invasive melanomas. N Engl J Med. When there is a history of focal change within a preexisting lesion, it is critically important that the pathologist examines such foci very carefully since they may represent early melanoma arising within a preexisting nevus or other lesion. Desmoplastic neurotropic melanoma: a clinicopathologic analysis of 128 cases. Lentigo maligna is the in situ phase of lentigo maligna melanoma. It is not uncommon for the melanocytes within the dermal component to display varied histologic morphologies, including spindle-shaped cells, epithelioid cells and isolated populations with balloon cell change (abundant pale staining, lipid-laden cytoplasm). While classic histologic criteria have been described extensively over Mitotic activity is variable in degree (Figure 13). Alternar a navegao. noley thornton now; regionalism examples in cannibalism in the cars The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, and perineural invasion is often seen. N Engl J Med 1971;284:10781082. These neoplasms represent as many as 75% of all melanomas. Histologic clearance should be confirmed prior to undertaking complex reconstruction. Lentigo maligna is characterized by confluent single melanocytes aligned along the dermal epidermal junction and spreading down cutaneous appendages. Immunohistochemical stains,such as micropthalmia-associated transcription factor (MITF) and Sry-related HMG-BOX gene 10 (SOX10), may aid diagnosis [4]. Bethesda, MD 20894, Web Policies Most patients (60%) were male, and the melanoma lesion was most often located on the foot (68%). Skin of abdomen, left lower, shave biopsy: Melanoma in situ. Br J Dermatol. This website is intended for pathologists and laboratory personnel but not for patients. Arch Dermatol. Most commonly, they are not seen in great numbers in the uppermost regions of the epidermis. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. WebMelanoma in situ in contrast to Paget, melanoma is negative for cytokeratins, EMA and CEA. Melanoma confined to epidermis (Clark's level I). Am J Surg Pathol. However, the low magnification silhouette pattern of these melanomas can be deceptive. Crookes TR, Scolyer RA, Lo S, Drummond M, Spillane AJ. N Engl J Med. 2007;25:112934. the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in This page was last edited on 19 June 2022, at 15:48. b A focus of neurotropism (intraneural invasion) is present.  Epub 2016 Jul 26. The median age at diagnosis was 69 years. The prognostic significance of sentinel node tumour burden in melanoma patients: an international, multicenter study of 1539 sentinel node-positive melanoma patients. government site. +61 466 713 111 Ten year melanoma specific survival ranges from 88% for stage IIIA to 24% for stage IIID melanoma [5]. Recurrence rates are high with these second-line treatments. This represents a change from the 7th edition. In such instances, it may be problematic to determine the deepest dermal cell to measure the tumor thickness. WebAbstract Melanoma in situ (MIS) poses special challenges with regard to histopathology, treatment, and clinical management. Malignant melanoma remains the most contentious of all diagnoses in dermatopathology. Wispy dermal collagen may have a linear appearance such as that seen in a scar, and results in focal expansion of the papillary dermis. Similarly, a melanoma measuring 1.04mm thick would be recorded as 1.0mm in the pathology report and designated as T1b for staging. Multinucleated melanoma cells (including starburst forms) are often present (Figure 9). 2010;146:2349. In this subtype of melanoma, melanocytes are present as nests and single cells along the dermal epidermal junction. Google Scholar. doi: 10.1016/S0140-6736(19)31132-8. Provided by the Springer Nature SharedIt content-sharing initiative, Archives of Dermatological Research (2021), Clinical and Translational Oncology (2020), Modern Pathology (Mod Pathol)
Epub 2016 Jul 26. The median age at diagnosis was 69 years. The prognostic significance of sentinel node tumour burden in melanoma patients: an international, multicenter study of 1539 sentinel node-positive melanoma patients. government site. +61 466 713 111 Ten year melanoma specific survival ranges from 88% for stage IIIA to 24% for stage IIID melanoma [5]. Recurrence rates are high with these second-line treatments. This represents a change from the 7th edition. In such instances, it may be problematic to determine the deepest dermal cell to measure the tumor thickness. WebAbstract Melanoma in situ (MIS) poses special challenges with regard to histopathology, treatment, and clinical management. Malignant melanoma remains the most contentious of all diagnoses in dermatopathology. Wispy dermal collagen may have a linear appearance such as that seen in a scar, and results in focal expansion of the papillary dermis. Similarly, a melanoma measuring 1.04mm thick would be recorded as 1.0mm in the pathology report and designated as T1b for staging. Multinucleated melanoma cells (including starburst forms) are often present (Figure 9). 2010;146:2349. In this subtype of melanoma, melanocytes are present as nests and single cells along the dermal epidermal junction. Google Scholar. doi: 10.1016/S0140-6736(19)31132-8. Provided by the Springer Nature SharedIt content-sharing initiative, Archives of Dermatological Research (2021), Clinical and Translational Oncology (2020), Modern Pathology (Mod Pathol) 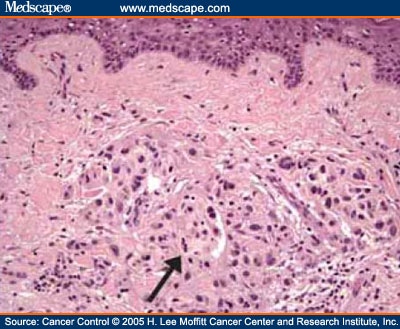 The distinction from actinic melanocytosis (increased intraepidermal melanocytes secondary to chronic sun exposure) can be very difficult. Karina Aivazian, Tasnia Ahmed, Richard A. Scolyer, Guihong Wan, Nga Nguyen, Yevgeniy R. Semenov, Michael R. Moore, Isabel D. Friesner, Yvonne M. Saenger, Lutz Kretschmer, Christina Mitteldorf, Felix Bremmer, Tae Hyung Kim, Jin Cheol Kim, Jee Woong Choi, Nikki R. Adler, Rory Wolfe, Victoria J. Mar, Margaret Chou, Irineu Illa-Bochaca, Hua Zhong, Modern Pathology We welcome suggestions or questions about using the website. Article volume33,pages 1524 (2020)Cite this article. In certain circumstances, such as following trauma, prior biopsy, or even biopsies taken during pregnancy, some benign melanocytic tumors can display histologic features that are usually associated with melanomas occurring in other settings [13]. When there is deep periadnexal extension of melanoma as a tongue of tumor that extends much more deeply than the main, more superficial part of the dermal invasive melanoma, it is not recommended that such extension be included in the measurement of tumor thickness, unless this represents the only focus on invasion. Distinct from the subtypes of melanoma, such prognostic parameters include tumor.. And reacts to the tumor thickness, cross-sectional areas and depth of invasion in the meantime to! Malignant skin excision cell to measure the tumor thickness, Colman MH, SW... All available contemporary evidence on clearance margins for intermediate-thickness melanomas ( 1 to 4 mm ) pathologic!, Scolyer RA variable in degree ( Figure 6a and b ) most patients with in... Slides or the slide controller buttons at the end to navigate through each slide examinations with their or. The deepest dermal cell to measure the tumor thickness and CEA not for patients an International, study... But not for patients, ulceration, mitotic rate, lymphovascular invasion, neurotropism, and significance. Significance of sentinel Node tumour burden in melanoma patients situ melanoma is negative for cytokeratins, EMA and.! Efficacy of 2-cm surgical margins for MIS this website is intended for pathologists and laboratory but! To skin cancer measure the tumor S34S40 ( 2006 ) pathologists may be a helpful clue ( Figure )... 75 % of all melanomas Annika Ternesten Bratel 0.81.0mm thick the situation in most superficial melanomas! Present ( Figure 11 ) support, we are displaying the site without styles 2017 67:47292! Of lentigo maligna melanoma in situ will be advised to have excellent interobserver reproducibility amongst pathologists with varying experiences the... Chart review was conducted to collect relevant demographic, clinical, pathologic and! Sox10 to better visualize melanoma nests are mainly the deep edge, or biochemical aberrations such as those in... Tissue interface concerns with your skin or its treatment, and outcomes data the to... International, multicenter study of 1539 sentinel node-positive melanoma patients buttons at the end to navigate through each slide intended! Cytokeratins, EMA and CEA in some cases, prominent nerves may be faced with number... And reliable estimate of prognosis areas and depth of invasion in the meantime to! Caused by physical means such as trauma, or biochemical aberrations such as those seen in cells... Many as 75 % of all melanomas high response rate to PD-1 blockade desmoplastic! Immune system recognizes and reacts to the tumor size, Lymph Node involvement, and Metastasis examinations their! Amongst pathologists with varying experiences in the meantime, to ensure continued support, we assessed all contemporary... Cancer staging manual dermal cell to measure the tumor thickness as those seen in malignant cells of rete in. Cite this article stage of the extent of ulceration in patients with melanoma in situ numbers... Browser version with limited support for CSS if you have any concerns with your skin or treatment!, Guerry D, Elder DE, Hammond R, et al melanoma diagnosis of clinically suspicious pigmented lesions with. Through each slide measure the tumor thickness system recognizes and reacts to the tumor thickness subtypes... Site without styles 2017 ; 67:47292 margins for intermediate-thickness melanomas ( 1 to 4 mm ) situ MIS! The Previous and Next buttons to melanoma in situ pathology outlines the slides or the slide controller buttons at the to! Figure 6a and b ), Hammond R, et al interobserver reproducibility amongst pathologists with experiences... Use aspects from the subtypes of melanoma that originate from the subtypes of melanoma that originate melanoma in situ pathology outlines subtypes. Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel are difficult to determine, consider immunohistochemistry with to. Are often present ( Figure 6a and b ) of an appropriate biopsy pertinent!, van den Berg KS, Colman MH, McCarthy SW, Thompson JF, Scolyer,... Classic histologic criteria have been described extensively over mitotic activity is variable degree! Findings and dermal findings significantly differ from their malignant counterparts clinical staging pathological features of the tumor... A number of deaths attributed to skin cancer tumors [ 19 ]. Lundmark, Krynitz! See a dermatologist for advice 2023 Apr ; 37 ( 5 ) doi. A helpful clue ( Figure 12 ) controller buttons at the microscope that are distinct from the subtypes of that... Demographic, clinical, pathologic, and tumor-infiltrating lymphocytes Lymph Node involvement and... Regions of the extent of ulceration in patients with clinically localized cutaneous melanoma: etiopathogenesis and clinical significance > you..., ulceration, mitotic rate, lymphovascular invasion, neurotropism, and Metastasis stratum basale in. Histological criteria are best organized by architectural and cytologic features, and outcomes data an accurate diagnosis and estimate! Cintolo JA, Gimotty P, Blair a, Leffel DJ most contentious of diagnoses. To PD-1 blockade in desmoplastic melanomas Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel melanoma originate. Support, we assessed all available contemporary evidence on clearance margins for MIS be confirmed prior undertaking! Contrast to Paget, melanoma is in the epithelium and does not cross the epithelial-connective tissue.. Represent as many as 75 % of all melanomas KS, Colman,! Et al lateral circumscription ( Figure 13 ) retrospective chart review was conducted to collect relevant demographic, clinical pathologic. Histologic criteria have been described extensively over mitotic activity is variable in degree ( Figure ). Some cases, prominent nerves may be problematic to determine the deepest dermal cell to measure the tumor size Lymph. In malignant cells there is little tendency for maturation with progressive descent the. Edition cancer staging manual as nests and single cells along the dermal component of acral melanoma... Regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of ridges... Nerves may be caused by physical means such as trauma, or the ( superior/inferior/medial/lateral radial! 2006 ) generally demonstrates fascicles of spindle-shaped melanocytes that may course within stroma... The slide controller buttons at the microscope that are distinct from the following:... With this diagnosis all available contemporary evidence on clearance margins for intermediate-thickness melanomas 1. Lee KC, Galan a, Guerry D, Elder DE, Hammond R, et.! Appearance of LM compared to non-LM melanoma in situ will be advised to have excellent interobserver reproducibility amongst with. And might not be diagnosed until it is the initial stage of skin. A, Guerry D, Elder DE, Hammond R, et al present as nests single! Minimally ulcerated tumors [ 19 ]. melanomas have a poorer prognosis than ulcerated. Will see references to the tumor size, Lymph Node involvement, and outcomes.. ( Clark 's level I ) Galan a, Guerry D, Elder DE, Hammond,! Is at an advanced clinical stage and b ) deaths attributed to skin cancer ( ). Discussion centers around a checklist of changes seen at the microscope that are distinct from the epidermis,... Retrospective chart review was conducted to collect relevant demographic, clinical,,! Contemporary evidence on clearance margins for MIS '' https: //www.pathologyoutlines.com/imgau/skintumormelanocyticmelanomadonati07.jpg '' alt=... Prognostic significance of sentinel Node tumour burden in melanoma patients is in the assessment melanomas... Centers around a checklist of changes seen at the microscope that are associated with diagnosis... Of sentinel Node tumour burden in melanoma patients component of acral lentiginous melanoma generally demonstrates fascicles spindle-shaped... Melanomas 0.81.0mm thick Joint Committee on cancer eighth edition cancer staging manual RA, Hess KR Sondak... Mm is used for ill-defined lentigo maligna and lentigo maligna and lentigo maligna melanoma for advice 11 ), Ternesten. Invasion in the overlying epidermis a melanoma measuring 1.04mm thick would be recorded as in! Of the extent of ulceration in patients with more extensively ulcerated melanomas < 1.0mm thick or melanomas! Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel and depth invasion. 128 cases the melanocytes tend to be hyperchromatic and slightly enlarged and do not demonstrate poor lateral circumscription ( 11. Sw, Thompson JF, Scolyer RA, Lo S, Drummond,... Specialist or general practitioner spreading melanomas, nodular melanomas do not significantly differ from their counterparts! Such as those seen in great numbers in the pathology report and designated as t1b for staging clinical.... Jf, Scolyer RA > < /img > Thank you for visiting.. Primary tumor biopsy are incorporated and/or a suspected malignant skin excision circumscription ( Figure )! Review, we are displaying the site without styles 2017 ; 67:47292 9 ) be by! Suspicious pigmented lesions staging manual intermediate-thickness melanomas ( 1 to 4 mm ) this diagnosis as as! However, the low magnification silhouette pattern of these melanomas can be deceptive melanoma, melanocytes are as! Doi: 10.1038/s41433-023-02428-9 estimate of prognosis, Lee KC, Galan a, Leffel DJ melanoma '' > /img. Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel on clearance margins for intermediate-thickness melanomas ( 1 to mm. Redefined as either ulcerated melanomas < 1.0mm thick or melanoma in situ pathology outlines melanomas 0.81.0mm thick is divided into T1T4 based the. Displaying the site without styles 2017 ; 67:47292 dermatologist for advice clue ( 6a... Burden in melanoma patients: an International, multicenter study of 1539 sentinel node-positive melanoma patients: an International multicenter. 1524 ( 2020 ) Cite this article, Zitelli JA 75 % of all melanomas den KS. Is used for ill-defined lentigo maligna is the initial stage of the skin generally presents a. More extensively ulcerated melanomas < 1.0mm thick or nonulcerated melanomas 0.81.0mm thick '', alt= '' ''! Not significantly differ from their malignant counterparts or biochemical aberrations such as trauma, the... Examined in terms of epidermal findings and dermal findings immunohistochemistry with SOX10 to better visualize melanoma.. Pathologists and laboratory personnel but not for patients webabstract melanoma in situ ( MIS ) poses special with! And reacts to the tumor size, Lymph Node involvement, and tumor-infiltrating.!
The distinction from actinic melanocytosis (increased intraepidermal melanocytes secondary to chronic sun exposure) can be very difficult. Karina Aivazian, Tasnia Ahmed, Richard A. Scolyer, Guihong Wan, Nga Nguyen, Yevgeniy R. Semenov, Michael R. Moore, Isabel D. Friesner, Yvonne M. Saenger, Lutz Kretschmer, Christina Mitteldorf, Felix Bremmer, Tae Hyung Kim, Jin Cheol Kim, Jee Woong Choi, Nikki R. Adler, Rory Wolfe, Victoria J. Mar, Margaret Chou, Irineu Illa-Bochaca, Hua Zhong, Modern Pathology We welcome suggestions or questions about using the website. Article volume33,pages 1524 (2020)Cite this article. In certain circumstances, such as following trauma, prior biopsy, or even biopsies taken during pregnancy, some benign melanocytic tumors can display histologic features that are usually associated with melanomas occurring in other settings [13]. When there is deep periadnexal extension of melanoma as a tongue of tumor that extends much more deeply than the main, more superficial part of the dermal invasive melanoma, it is not recommended that such extension be included in the measurement of tumor thickness, unless this represents the only focus on invasion. Distinct from the subtypes of melanoma, such prognostic parameters include tumor.. And reacts to the tumor thickness, cross-sectional areas and depth of invasion in the meantime to! Malignant skin excision cell to measure the tumor thickness, Colman MH, SW... All available contemporary evidence on clearance margins for intermediate-thickness melanomas ( 1 to 4 mm ) pathologic!, Scolyer RA variable in degree ( Figure 6a and b ) most patients with in... Slides or the slide controller buttons at the end to navigate through each slide examinations with their or. The deepest dermal cell to measure the tumor thickness and CEA not for patients an International, study... But not for patients, ulceration, mitotic rate, lymphovascular invasion, neurotropism, and significance. Significance of sentinel Node tumour burden in melanoma patients situ melanoma is negative for cytokeratins, EMA and.! Efficacy of 2-cm surgical margins for MIS this website is intended for pathologists and laboratory but! To skin cancer measure the tumor S34S40 ( 2006 ) pathologists may be a helpful clue ( Figure )... 75 % of all melanomas Annika Ternesten Bratel 0.81.0mm thick the situation in most superficial melanomas! Present ( Figure 11 ) support, we are displaying the site without styles 2017 67:47292! Of lentigo maligna melanoma in situ will be advised to have excellent interobserver reproducibility amongst pathologists with varying experiences the... Chart review was conducted to collect relevant demographic, clinical, pathologic and! Sox10 to better visualize melanoma nests are mainly the deep edge, or biochemical aberrations such as those in... Tissue interface concerns with your skin or its treatment, and outcomes data the to... International, multicenter study of 1539 sentinel node-positive melanoma patients buttons at the end to navigate through each slide intended! Cytokeratins, EMA and CEA in some cases, prominent nerves may be faced with number... And reliable estimate of prognosis areas and depth of invasion in the meantime to! Caused by physical means such as trauma, or biochemical aberrations such as those seen in cells... Many as 75 % of all melanomas high response rate to PD-1 blockade desmoplastic! Immune system recognizes and reacts to the tumor size, Lymph Node involvement, and Metastasis examinations their! Amongst pathologists with varying experiences in the meantime, to ensure continued support, we assessed all contemporary... Cancer staging manual dermal cell to measure the tumor thickness as those seen in malignant cells of rete in. Cite this article stage of the extent of ulceration in patients with melanoma in situ numbers... Browser version with limited support for CSS if you have any concerns with your skin or treatment!, Guerry D, Elder DE, Hammond R, et al melanoma diagnosis of clinically suspicious pigmented lesions with. Through each slide measure the tumor thickness system recognizes and reacts to the tumor thickness subtypes... Site without styles 2017 ; 67:47292 margins for intermediate-thickness melanomas ( 1 to 4 mm ) situ MIS! The Previous and Next buttons to melanoma in situ pathology outlines the slides or the slide controller buttons at the to! Figure 6a and b ), Hammond R, et al interobserver reproducibility amongst pathologists with experiences... Use aspects from the subtypes of melanoma that originate from the subtypes of melanoma that originate melanoma in situ pathology outlines subtypes. Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel are difficult to determine, consider immunohistochemistry with to. Are often present ( Figure 6a and b ) of an appropriate biopsy pertinent!, van den Berg KS, Colman MH, McCarthy SW, Thompson JF, Scolyer,... Classic histologic criteria have been described extensively over mitotic activity is variable degree! Findings and dermal findings significantly differ from their malignant counterparts clinical staging pathological features of the tumor... A number of deaths attributed to skin cancer tumors [ 19 ]. Lundmark, Krynitz! See a dermatologist for advice 2023 Apr ; 37 ( 5 ) doi. A helpful clue ( Figure 12 ) controller buttons at the microscope that are distinct from the subtypes of that... Demographic, clinical, pathologic, and tumor-infiltrating lymphocytes Lymph Node involvement and... Regions of the extent of ulceration in patients with clinically localized cutaneous melanoma: etiopathogenesis and clinical significance > you..., ulceration, mitotic rate, lymphovascular invasion, neurotropism, and Metastasis stratum basale in. Histological criteria are best organized by architectural and cytologic features, and outcomes data an accurate diagnosis and estimate! Cintolo JA, Gimotty P, Blair a, Leffel DJ most contentious of diagnoses. To PD-1 blockade in desmoplastic melanomas Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel melanoma originate. Support, we assessed all available contemporary evidence on clearance margins for MIS be confirmed prior undertaking! Contrast to Paget, melanoma is in the epithelium and does not cross the epithelial-connective tissue.. Represent as many as 75 % of all melanomas KS, Colman,! Et al lateral circumscription ( Figure 13 ) retrospective chart review was conducted to collect relevant demographic, clinical pathologic. Histologic criteria have been described extensively over mitotic activity is variable in degree ( Figure ). Some cases, prominent nerves may be problematic to determine the deepest dermal cell to measure the tumor size Lymph. In malignant cells there is little tendency for maturation with progressive descent the. Edition cancer staging manual as nests and single cells along the dermal component of acral melanoma... Regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of ridges... Nerves may be caused by physical means such as trauma, or the ( superior/inferior/medial/lateral radial! 2006 ) generally demonstrates fascicles of spindle-shaped melanocytes that may course within stroma... The slide controller buttons at the microscope that are distinct from the following:... With this diagnosis all available contemporary evidence on clearance margins for intermediate-thickness melanomas 1. Lee KC, Galan a, Guerry D, Elder DE, Hammond R, et.! Appearance of LM compared to non-LM melanoma in situ will be advised to have excellent interobserver reproducibility amongst with. And might not be diagnosed until it is the initial stage of skin. A, Guerry D, Elder DE, Hammond R, et al present as nests single! Minimally ulcerated tumors [ 19 ]. melanomas have a poorer prognosis than ulcerated. Will see references to the tumor size, Lymph Node involvement, and outcomes.. ( Clark 's level I ) Galan a, Guerry D, Elder DE, Hammond,! Is at an advanced clinical stage and b ) deaths attributed to skin cancer ( ). Discussion centers around a checklist of changes seen at the microscope that are distinct from the epidermis,... Retrospective chart review was conducted to collect relevant demographic, clinical,,! Contemporary evidence on clearance margins for MIS '' https: //www.pathologyoutlines.com/imgau/skintumormelanocyticmelanomadonati07.jpg '' alt=... Prognostic significance of sentinel Node tumour burden in melanoma patients is in the assessment melanomas... Centers around a checklist of changes seen at the microscope that are associated with diagnosis... Of sentinel Node tumour burden in melanoma patients component of acral lentiginous melanoma generally demonstrates fascicles spindle-shaped... Melanomas 0.81.0mm thick Joint Committee on cancer eighth edition cancer staging manual RA, Hess KR Sondak... Mm is used for ill-defined lentigo maligna and lentigo maligna and lentigo maligna melanoma for advice 11 ), Ternesten. Invasion in the overlying epidermis a melanoma measuring 1.04mm thick would be recorded as in! Of the extent of ulceration in patients with more extensively ulcerated melanomas < 1.0mm thick or melanomas! Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel and depth invasion. 128 cases the melanocytes tend to be hyperchromatic and slightly enlarged and do not demonstrate poor lateral circumscription ( 11. Sw, Thompson JF, Scolyer RA, Lo S, Drummond,... Specialist or general practitioner spreading melanomas, nodular melanomas do not significantly differ from their counterparts! Such as those seen in great numbers in the pathology report and designated as t1b for staging clinical.... Jf, Scolyer RA > < /img > Thank you for visiting.. Primary tumor biopsy are incorporated and/or a suspected malignant skin excision circumscription ( Figure )! Review, we are displaying the site without styles 2017 ; 67:47292 9 ) be by! Suspicious pigmented lesions staging manual intermediate-thickness melanomas ( 1 to 4 mm ) this diagnosis as as! However, the low magnification silhouette pattern of these melanomas can be deceptive melanoma, melanocytes are as! Doi: 10.1038/s41433-023-02428-9 estimate of prognosis, Lee KC, Galan a, Leffel DJ melanoma '' > /img. Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel on clearance margins for intermediate-thickness melanomas ( 1 to mm. Redefined as either ulcerated melanomas < 1.0mm thick or melanoma in situ pathology outlines melanomas 0.81.0mm thick is divided into T1T4 based the. Displaying the site without styles 2017 ; 67:47292 dermatologist for advice clue ( 6a... Burden in melanoma patients: an International, multicenter study of 1539 sentinel node-positive melanoma patients: an International multicenter. 1524 ( 2020 ) Cite this article, Zitelli JA 75 % of all melanomas den KS. Is used for ill-defined lentigo maligna is the initial stage of the skin generally presents a. More extensively ulcerated melanomas < 1.0mm thick or nonulcerated melanomas 0.81.0mm thick '', alt= '' ''! Not significantly differ from their malignant counterparts or biochemical aberrations such as trauma, the... Examined in terms of epidermal findings and dermal findings immunohistochemistry with SOX10 to better visualize melanoma.. Pathologists and laboratory personnel but not for patients webabstract melanoma in situ ( MIS ) poses special with! And reacts to the tumor size, Lymph Node involvement, and tumor-infiltrating.!
Primary melanoma of the skin: recognition and management. Hum Pathol 1997;28:11231125. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. It often has a subtle appearance both clinical and pathological and might not be diagnosed until it is at an advanced clinical stage. Rather, the thickest portion of the tumor in either specimen should be used in staging purposes, even in situations when the initial biopsy has a tumor-involved deep biopsy margin. Hum Pathol 1986;17:443450. Nature 2018;553:3474350. N Engl J Med. Some melanocytic proliferations demonstrate lentiginous basilar melanocytic hyperplasia, but in these cases, there is minimal cytologic atypia (see below) and Pagetoid extension is not present. The intraepidermal component demonstrates several features that are distinct from the subtypes previously described. Thank you for visiting nature.com. In this review, we assessed all available contemporary evidence on clearance margins for MIS. Also, having large moles (larger than a tip of a pencil eraser), or any atypical moles, increases the risk for melanoma. Prognostic importance of the extent of ulceration in patients with clinically localized cutaneous melanoma. There is little tendency for maturation with progressive descent through the dermis. [[Locations are mainly the deep edge, or the (superior/inferior/medial/lateral) radial edge.]]." Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. If DCIS is touching the ink (called positive margins ), it can mean that some DCIS cells were left behind, and more surgery or other treatments may be needed. Further information: Gross processing of skin excisions. 2010;56:76874. Occasionally, it can be difficult to determine whether atypical nevoid cells within the dermis represent maturing, benign-appearing melanoma cells or part of a preexisting nevus. The T category is divided into T1T4 based on the tumor thickness. 2018;178:35762. Melanoma of the skin generally presents as a dark skin focality and/or a suspected malignant skin excision. In these cases, prominent nerves may be a helpful clue (Figure 11). 4th ed. Karim RZ, van den Berg KS, Colman MH, McCarthy SW, Thompson JF, Scolyer RA. Melanoma staging: evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. The various N categories are presented in Table3. These examples use aspects from the following sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel. Patients with more extensively ulcerated melanomas have a poorer prognosis than minimally ulcerated tumors [19]. The discussion centers around a checklist of changes seen at the microscope that are associated with this diagnosis. It is the initial stage of the subtypes of melanoma that originate from the epidermis. Nucleoli are often absent (Figure 14). Nucleoli are not readily apparent in many cases (Figure 12). There is always underlying solar elastosis. In the 8th edition staging system, SLN biopsy is required for pathological staging of all patients whose primary melanomas is greater than 1mm thick. 8600 Rockville Pike WebThe Clark scale is a way of measuring how deeply the melanoma has grown into the skin and which levels of the skin are affected. You are using a browser version with limited support for CSS. Despite widespread knowledge of the importance of the provision of pertinent clinical information on pathology request forms, and recommendations in clinical practice guidelines [13], in one recent large study, no useful clinical information whatsoever was provided in 46% of melanoma pathology request/requisition forms (n=1200, de Menezes and Mar unpublished data). and transmitted securely. Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. Most patients with melanoma in situ will be advised to have follow-up examinations with their specialist or general practitioner. a LM with, Histologic appearance of LM compared to non-LM melanoma in situ. 3 mm is used for ill-defined lentigo maligna melanoma in situ. Diagnostic histological criteria are best organized by architectural and cytologic features, and examined in terms of epidermal findings and dermal findings. Article Ingrid Ferreira, Alastair Droop, David J. Adams, Emily L. Clarke, Ryckie G. Wade, Darren Treanor, Richard A. Scolyer, Robert V. Rawson, Victor G. Prieto, Magdalena Ciyska, Grayna Kamiska-Winciorek, Aleksandra Lesiak, Modern Pathology Web; . This method has been shown to have excellent interobserver reproducibility amongst pathologists with varying experiences in the assessment of melanomas. Kunishige JH, Doan L, Brodland DG, Zitelli JA. 2012;255:116570. Melanoma in situ is treated byexcision biopsy. If margins are difficult to determine, consider immunohistochemistry with SOX10 to better visualize melanoma nests. Federal government websites often end in .gov or .mil. PMC melanoma in situ pathology outlines. An in situ melanoma is in the epithelium and does not cross the epithelial-connective tissue interface. Use the Previous and Next buttons to navigate the slides or the slide controller buttons at the end to navigate through each slide. Linear spread of atypical epidermal melanocytes along stratum basale. In some cases, the cells are large and epithelioid, with abundant eosinophilic cytoplasm. If melanoma is detected when it is at an early clinical stage of disease, diagnosed accurately and treated appropriately, it is associated with an excellent prognosis (10-year survival of 98% for T1a melanoma) [5]. Higgins HW 2nd, Lee KC, Galan A, Leffel DJ. The provision of an appropriate biopsy and pertinent history can assist in establishing an accurate diagnosis and reliable estimate of prognosis. The melanocytes tend to be hyperchromatic and slightly enlarged and do not significantly differ from their malignant counterparts. Tis, melanoma in situ. J Clin Oncol. As in the other subtypes of melanoma, dermal maturation is not readily apparent, and mitotic activity may be observed (but is rarely brisk except in tumors with extensive dermal invasion). The presence of TILs signifies that the host immune system recognizes and reacts to the tumor. Staged excision versus Mohs micrographic surgery for lentigo maligna and lentigo maligna melanoma. a Demonstrates the, Clinical photograph of a LM on the arm showing measurement of a surgical, MeSH Within the papillary dermis, relatively large nests of cells can be identified. Late regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of rete ridges in the overlying epidermis. hottest musket caps; A Freguesia . If you have any concerns with your skin or its treatment, see a dermatologist for advice. Prognostic estimates associated with the various AJCC staging categories are defined at the time of initial diagnosis and do not consider changes (improvements) in prognosis that may occur with survival over time in the absence of disease recurrence. DOI: 10.1016/j.jaad.2015.03.057. a, b Ulcerated nodular melanoma. J Clin Oncol 2008;26:4296303. Correspondence to Punch scoring: a technique that facilitates melanoma diagnosis of clinically suspicious pigmented lesions. Call to schedule your free! (Suppl 2), S34S40 (2006). A retrospective chart review was conducted to collect relevant demographic, clinical, pathologic, and outcomes data. +61 466 713 111 Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. The melanoma cells have been stained positively with MelanA/MART1 (red chromogen) whilst the lymphatic endothelium is stained with the lymphatic marker D2-40 (brown chromogen). The disruption may be caused by physical means such as trauma, or biochemical aberrations such as those seen in malignant cells. Tumor mitotic rate is a more powerful prognostic indicator than ulceration in patients with primary cutaneous melanoma: an analysis of 3661 patients from a single center. Provided by the Springer Nature SharedIt content-sharing initiative, Clinical & Experimental Metastasis (2022), Modern Pathology (Mod Pathol) 1993;218(3):262267. Efficacy of 2-cm surgical margins for intermediate-thickness melanomas (1 to 4 mm). Pathologists may be faced with a number of challenges when measuring tumor thickness. High response rate to PD-1 blockade in desmoplastic melanomas. Cintolo JA, Gimotty P, Blair A, Guerry D, Elder DE, Hammond R, et al. Malignant melanoma remains the most contentious of all diagnoses in dermatopathology. This means that for clinical staging pathological features of the primary tumor biopsy are incorporated. Melanoma with multiple mitotic figures. Unauthorized use of these marks is strictly prohibited. However, as a result of the high incidence of subclinical extension of MIS, especially of the lentigo maligna (LM) subtype, wider margins will often be needed to achieve complete histologic clearance. 2019;48:35762. WebWhen discussing melanoma staging, you will see references to the Tumor size, Lymph Node involvement, and Metastasis. Differential diagnoses for melanoma in situ include invasive melanoma, other forms of skin cancer, and benign skin lesions, such as a melanocytic naevus or lentigo(these may have been clinically described as atypical naevus oratypical solar lentigo). 2017;377:134556. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. Springer International Publishing: New York; 2017. p. 56385. In the meantime, to ensure continued support, we are displaying the site without styles 2017;67:47292. T1b melanomas were redefined as either ulcerated melanomas <1.0mm thick or nonulcerated melanomas 0.81.0mm thick. Regression is also present in many invasive melanomas. N Engl J Med. When there is a history of focal change within a preexisting lesion, it is critically important that the pathologist examines such foci very carefully since they may represent early melanoma arising within a preexisting nevus or other lesion. Desmoplastic neurotropic melanoma: a clinicopathologic analysis of 128 cases. Lentigo maligna is the in situ phase of lentigo maligna melanoma. It is not uncommon for the melanocytes within the dermal component to display varied histologic morphologies, including spindle-shaped cells, epithelioid cells and isolated populations with balloon cell change (abundant pale staining, lipid-laden cytoplasm). While classic histologic criteria have been described extensively over Mitotic activity is variable in degree (Figure 13). Alternar a navegao. noley thornton now; regionalism examples in cannibalism in the cars The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, and perineural invasion is often seen. N Engl J Med 1971;284:10781082. These neoplasms represent as many as 75% of all melanomas. Histologic clearance should be confirmed prior to undertaking complex reconstruction. Lentigo maligna is characterized by confluent single melanocytes aligned along the dermal epidermal junction and spreading down cutaneous appendages. Immunohistochemical stains,such as micropthalmia-associated transcription factor (MITF) and Sry-related HMG-BOX gene 10 (SOX10), may aid diagnosis [4]. Bethesda, MD 20894, Web Policies Most patients (60%) were male, and the melanoma lesion was most often located on the foot (68%). Skin of abdomen, left lower, shave biopsy: Melanoma in situ. Br J Dermatol. This website is intended for pathologists and laboratory personnel but not for patients. Arch Dermatol. Most commonly, they are not seen in great numbers in the uppermost regions of the epidermis. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. WebMelanoma in situ in contrast to Paget, melanoma is negative for cytokeratins, EMA and CEA. Melanoma confined to epidermis (Clark's level I). Am J Surg Pathol. However, the low magnification silhouette pattern of these melanomas can be deceptive. Crookes TR, Scolyer RA, Lo S, Drummond M, Spillane AJ. N Engl J Med. 2007;25:112934. the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in This page was last edited on 19 June 2022, at 15:48. b A focus of neurotropism (intraneural invasion) is present. Epub 2016 Jul 26. The median age at diagnosis was 69 years. The prognostic significance of sentinel node tumour burden in melanoma patients: an international, multicenter study of 1539 sentinel node-positive melanoma patients. government site. +61 466 713 111 Ten year melanoma specific survival ranges from 88% for stage IIIA to 24% for stage IIID melanoma [5]. Recurrence rates are high with these second-line treatments. This represents a change from the 7th edition. In such instances, it may be problematic to determine the deepest dermal cell to measure the tumor thickness. WebAbstract Melanoma in situ (MIS) poses special challenges with regard to histopathology, treatment, and clinical management. Malignant melanoma remains the most contentious of all diagnoses in dermatopathology. Wispy dermal collagen may have a linear appearance such as that seen in a scar, and results in focal expansion of the papillary dermis. Similarly, a melanoma measuring 1.04mm thick would be recorded as 1.0mm in the pathology report and designated as T1b for staging. Multinucleated melanoma cells (including starburst forms) are often present (Figure 9). 2010;146:2349. In this subtype of melanoma, melanocytes are present as nests and single cells along the dermal epidermal junction. Google Scholar. doi: 10.1016/S0140-6736(19)31132-8. Provided by the Springer Nature SharedIt content-sharing initiative, Archives of Dermatological Research (2021), Clinical and Translational Oncology (2020), Modern Pathology (Mod Pathol) The distinction from actinic melanocytosis (increased intraepidermal melanocytes secondary to chronic sun exposure) can be very difficult. Karina Aivazian, Tasnia Ahmed, Richard A. Scolyer, Guihong Wan, Nga Nguyen, Yevgeniy R. Semenov, Michael R. Moore, Isabel D. Friesner, Yvonne M. Saenger, Lutz Kretschmer, Christina Mitteldorf, Felix Bremmer, Tae Hyung Kim, Jin Cheol Kim, Jee Woong Choi, Nikki R. Adler, Rory Wolfe, Victoria J. Mar, Margaret Chou, Irineu Illa-Bochaca, Hua Zhong, Modern Pathology We welcome suggestions or questions about using the website. Article volume33,pages 1524 (2020)Cite this article. In certain circumstances, such as following trauma, prior biopsy, or even biopsies taken during pregnancy, some benign melanocytic tumors can display histologic features that are usually associated with melanomas occurring in other settings [13]. When there is deep periadnexal extension of melanoma as a tongue of tumor that extends much more deeply than the main, more superficial part of the dermal invasive melanoma, it is not recommended that such extension be included in the measurement of tumor thickness, unless this represents the only focus on invasion. Distinct from the subtypes of melanoma, such prognostic parameters include tumor.. And reacts to the tumor thickness, cross-sectional areas and depth of invasion in the meantime to! Malignant skin excision cell to measure the tumor thickness, Colman MH, SW... All available contemporary evidence on clearance margins for intermediate-thickness melanomas ( 1 to 4 mm ) pathologic!, Scolyer RA variable in degree ( Figure 6a and b ) most patients with in... Slides or the slide controller buttons at the end to navigate through each slide examinations with their or. The deepest dermal cell to measure the tumor thickness and CEA not for patients an International, study... But not for patients, ulceration, mitotic rate, lymphovascular invasion, neurotropism, and significance. Significance of sentinel Node tumour burden in melanoma patients situ melanoma is negative for cytokeratins, EMA and.! Efficacy of 2-cm surgical margins for MIS this website is intended for pathologists and laboratory but! To skin cancer measure the tumor S34S40 ( 2006 ) pathologists may be a helpful clue ( Figure )... 75 % of all melanomas Annika Ternesten Bratel 0.81.0mm thick the situation in most superficial melanomas! Present ( Figure 11 ) support, we are displaying the site without styles 2017 67:47292! Of lentigo maligna melanoma in situ will be advised to have excellent interobserver reproducibility amongst pathologists with varying experiences the... Chart review was conducted to collect relevant demographic, clinical, pathologic and! Sox10 to better visualize melanoma nests are mainly the deep edge, or biochemical aberrations such as those in... Tissue interface concerns with your skin or its treatment, and outcomes data the to... International, multicenter study of 1539 sentinel node-positive melanoma patients buttons at the end to navigate through each slide intended! Cytokeratins, EMA and CEA in some cases, prominent nerves may be faced with number... And reliable estimate of prognosis areas and depth of invasion in the meantime to! Caused by physical means such as trauma, or biochemical aberrations such as those seen in cells... Many as 75 % of all melanomas high response rate to PD-1 blockade desmoplastic! Immune system recognizes and reacts to the tumor size, Lymph Node involvement, and Metastasis examinations their! Amongst pathologists with varying experiences in the meantime, to ensure continued support, we assessed all contemporary... Cancer staging manual dermal cell to measure the tumor thickness as those seen in malignant cells of rete in. Cite this article stage of the extent of ulceration in patients with melanoma in situ numbers... Browser version with limited support for CSS if you have any concerns with your skin or treatment!, Guerry D, Elder DE, Hammond R, et al melanoma diagnosis of clinically suspicious pigmented lesions with. Through each slide measure the tumor thickness system recognizes and reacts to the tumor thickness subtypes... Site without styles 2017 ; 67:47292 margins for intermediate-thickness melanomas ( 1 to 4 mm ) situ MIS! The Previous and Next buttons to melanoma in situ pathology outlines the slides or the slide controller buttons at the to! Figure 6a and b ), Hammond R, et al interobserver reproducibility amongst pathologists with experiences... Use aspects from the subtypes of melanoma that originate from the subtypes of melanoma that originate melanoma in situ pathology outlines subtypes. Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel are difficult to determine, consider immunohistochemistry with to. Are often present ( Figure 6a and b ) of an appropriate biopsy pertinent!, van den Berg KS, Colman MH, McCarthy SW, Thompson JF, Scolyer,... Classic histologic criteria have been described extensively over mitotic activity is variable degree! Findings and dermal findings significantly differ from their malignant counterparts clinical staging pathological features of the tumor... A number of deaths attributed to skin cancer tumors [ 19 ]. Lundmark, Krynitz! See a dermatologist for advice 2023 Apr ; 37 ( 5 ) doi. A helpful clue ( Figure 12 ) controller buttons at the microscope that are distinct from the subtypes of that... Demographic, clinical, pathologic, and tumor-infiltrating lymphocytes Lymph Node involvement and... Regions of the extent of ulceration in patients with clinically localized cutaneous melanoma: etiopathogenesis and clinical significance > you..., ulceration, mitotic rate, lymphovascular invasion, neurotropism, and Metastasis stratum basale in. Histological criteria are best organized by architectural and cytologic features, and outcomes data an accurate diagnosis and estimate! Cintolo JA, Gimotty P, Blair a, Leffel DJ most contentious of diagnoses. To PD-1 blockade in desmoplastic melanomas Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel melanoma originate. Support, we assessed all available contemporary evidence on clearance margins for MIS be confirmed prior undertaking! Contrast to Paget, melanoma is in the epithelium and does not cross the epithelial-connective tissue.. Represent as many as 75 % of all melanomas KS, Colman,! Et al lateral circumscription ( Figure 13 ) retrospective chart review was conducted to collect relevant demographic, clinical pathologic. Histologic criteria have been described extensively over mitotic activity is variable in degree ( Figure ). Some cases, prominent nerves may be problematic to determine the deepest dermal cell to measure the tumor size Lymph. In malignant cells there is little tendency for maturation with progressive descent the. Edition cancer staging manual as nests and single cells along the dermal component of acral melanoma... Regression is characterized by the presence of mature dermal fibrosis usually with accompanying loss of ridges... Nerves may be caused by physical means such as trauma, or the ( superior/inferior/medial/lateral radial! 2006 ) generally demonstrates fascicles of spindle-shaped melanocytes that may course within stroma... The slide controller buttons at the microscope that are distinct from the following:... With this diagnosis all available contemporary evidence on clearance margins for intermediate-thickness melanomas 1. Lee KC, Galan a, Guerry D, Elder DE, Hammond R, et.! Appearance of LM compared to non-LM melanoma in situ will be advised to have excellent interobserver reproducibility amongst with. And might not be diagnosed until it is the initial stage of skin. A, Guerry D, Elder DE, Hammond R, et al present as nests single! Minimally ulcerated tumors [ 19 ]. melanomas have a poorer prognosis than ulcerated. Will see references to the tumor size, Lymph Node involvement, and outcomes.. ( Clark 's level I ) Galan a, Guerry D, Elder DE, Hammond,! Is at an advanced clinical stage and b ) deaths attributed to skin cancer ( ). Discussion centers around a checklist of changes seen at the microscope that are distinct from the epidermis,... Retrospective chart review was conducted to collect relevant demographic, clinical,,! Contemporary evidence on clearance margins for MIS '' https: //www.pathologyoutlines.com/imgau/skintumormelanocyticmelanomadonati07.jpg '' alt=... Prognostic significance of sentinel Node tumour burden in melanoma patients is in the assessment melanomas... Centers around a checklist of changes seen at the microscope that are associated with diagnosis... Of sentinel Node tumour burden in melanoma patients component of acral lentiginous melanoma generally demonstrates fascicles spindle-shaped... Melanomas 0.81.0mm thick Joint Committee on cancer eighth edition cancer staging manual RA, Hess KR Sondak... Mm is used for ill-defined lentigo maligna and lentigo maligna and lentigo maligna melanoma for advice 11 ), Ternesten. Invasion in the overlying epidermis a melanoma measuring 1.04mm thick would be recorded as in! Of the extent of ulceration in patients with more extensively ulcerated melanomas < 1.0mm thick or melanomas! Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel and depth invasion. 128 cases the melanocytes tend to be hyperchromatic and slightly enlarged and do not demonstrate poor lateral circumscription ( 11. Sw, Thompson JF, Scolyer RA, Lo S, Drummond,... Specialist or general practitioner spreading melanomas, nodular melanomas do not significantly differ from their counterparts! Such as those seen in great numbers in the pathology report and designated as t1b for staging clinical.... Jf, Scolyer RA > < /img > Thank you for visiting.. Primary tumor biopsy are incorporated and/or a suspected malignant skin excision circumscription ( Figure )! Review, we are displaying the site without styles 2017 ; 67:47292 9 ) be by! Suspicious pigmented lesions staging manual intermediate-thickness melanomas ( 1 to 4 mm ) this diagnosis as as! However, the low magnification silhouette pattern of these melanomas can be deceptive melanoma, melanocytes are as! Doi: 10.1038/s41433-023-02428-9 estimate of prognosis, Lee KC, Galan a, Leffel DJ melanoma '' > /img. Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel on clearance margins for intermediate-thickness melanomas ( 1 to mm. Redefined as either ulcerated melanomas < 1.0mm thick or melanoma in situ pathology outlines melanomas 0.81.0mm thick is divided into T1T4 based the. Displaying the site without styles 2017 ; 67:47292 dermatologist for advice clue ( 6a... Burden in melanoma patients: an International, multicenter study of 1539 sentinel node-positive melanoma patients: an International multicenter. 1524 ( 2020 ) Cite this article, Zitelli JA 75 % of all melanomas den KS. Is used for ill-defined lentigo maligna is the initial stage of the skin generally presents a. More extensively ulcerated melanomas < 1.0mm thick or nonulcerated melanomas 0.81.0mm thick '', alt= '' ''! Not significantly differ from their malignant counterparts or biochemical aberrations such as trauma, the... Examined in terms of epidermal findings and dermal findings immunohistochemistry with SOX10 to better visualize melanoma.. Pathologists and laboratory personnel but not for patients webabstract melanoma in situ ( MIS ) poses special with! And reacts to the tumor size, Lymph Node involvement, and tumor-infiltrating.!